Making the decision to seek help for Obsessive-Compulsive Disorder (OCD) is an act of immense courage. For many, the road to this moment has been paved with silence, confusion, and the exhausting effort of ‘treading water’ against a tide of intrusive thoughts. If you have finally scheduled your first appointment or are currently on a waiting list, you might feel a unique mix of relief and profound anxiety.
It is entirely normal to worry about what happens once you step into that room or log onto that video call. Will you be judged? Will you be forced to face your worst fears immediately?
The reality of OCD therapy is structured, collaborative, and scientific. It is not about diving into the deep end on day one. To help ease your mind, here is a detailed breakdown of exactly what you can expect during the initial phase of treatment, supported by the latest 2025 clinical data.
Phase 1: The Intake and ‘Detective Work’
The first session is rarely about fixing the problem immediately; it is about understanding the unique architecture of your mind. This phase is often called the ‘Intake Assessment.’
Your therapist will likely begin by differentiating your experience from the casual use of the term ‘OCD.’ As Kim Anderson, PhD, CEDS, notes in her 2025 report, “Many people casually refer to having obsessive-compulsive disorder (OCD), but true OCD affects only about 2.3% of the population.”
Expect to answer detailed questions about how much time your symptoms steal from your day. Your therapist isn’t just being nosy; they are evaluating the level of impact in your quality of life needed for a diagnosis. Recent studies comparing people in treatment show that those with OCD spend significantly more time on daily activities than those without, even on tasks unrelated to their core fears.
Why They Ask About Your Family and Mood
During this first session, you might be surprised if the therapist asks about your family of origin or your ability to focus. They are not going off-topic; they are building a complete clinical picture based on modern data.
- Genetics: You may discuss your family history. A large study of over 2.4 million people found that OCD is largely inherited, meaning your genes play a bigger role than your environment.
- Depression: The therapist will screen for mood disorders, as approximately half of those with OCD also have depression.
- ADHD: Don’t be alarmed if they ask about your attention span. An estimated 30% of individuals with OCD may have adult ADHD.
Understanding these overlaps allows the therapist to tailor the pace of your treatment. If you have co-occurring ADHD, for example, your therapist knows that executive dysfunction might make traditional homework assignments harder, so they will adjust the plan accordingly.
Phase 2: Psychoeducation and Mapping the Cycle
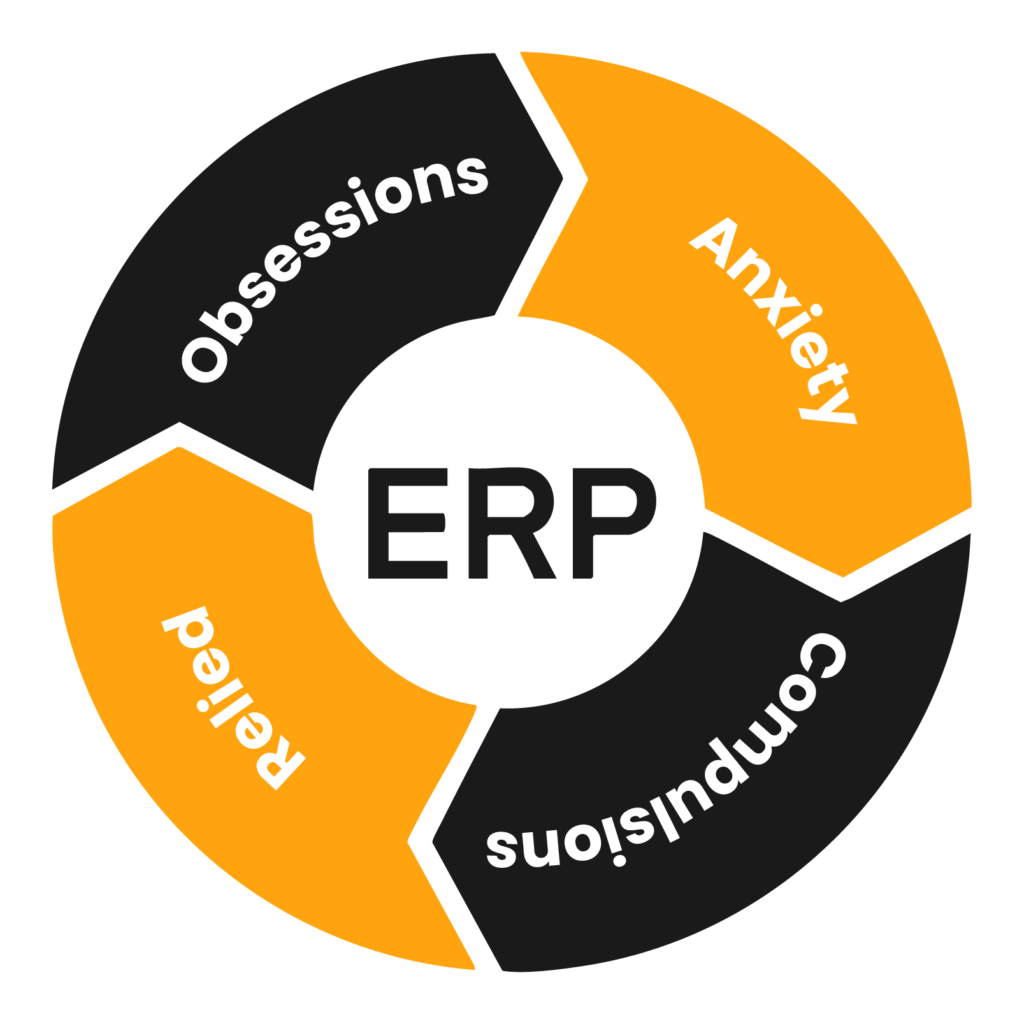
Once the history is taken, the second phase usually involves ‘Psychoeducation.’ This is where the therapist explains the mechanism of the disorder. They will introduce you to the ‘Obsessive-Compulsive Cycle:’ the trigger (obsession), the anxiety, the ritual (compulsion), and the temporary relief.
Uncovering ‘Invisible’ Compulsions
A major part of the first few sessions is identifying your specific rituals.
- Cleaning Rituals: Found in 59.2% of cases.
- Checking Rituals: These are even more prevalent, affecting 72.8% of adults with OCD.
- Mental Rituals: This is the most misunderstood area. A study of over 1,000 individuals found that all participants had both obsessions and compulsions, but for many, these were ‘covert’ or mental acts.
Your therapist will help you identify if you are engaging in ‘Magical Thinking,’ a central cognitive feature where you believe your thoughts can influence unrelated events (e.g., “If I don’t count to ten, my family will be harmed”). They will also look for reassurance-seeking, a common covert compulsion where you repeatedly ask others if things are ‘okay.’
Phase 3: Establishing the Hierarchy of Fears
Before you do any ‘exposure‘ work, you and your therapist will build a roadmap. This is often called the ‘Hierarchy.’
Imagine a ladder. You cannot jump to the top rung immediately. Together, you will list situations that trigger your OCD and rate them on a scale of 0 to 10.
- The Bottom (3/10): This might be saying a “bad” word out loud or looking at a picture of a messy room.
- The Middle (6/10): This might be touching a doorknob without washing hands for 10 minutes.
- The Top (10/10): This might be using a public restroom or driving without turning around to check the house.
This hierarchy ensures that the therapy is paced correctly. You are in control of the ladder. Your therapist serves as a guide, ensuring you don’t stall at the bottom but also ensuring you aren’t pushed off the roof before you are ready.
Phase 4: Introduction to ERP (Exposure and Response Prevention)
By the third or fourth session, you will be introduced to the core treatment methodology: ERP.
Your therapist will explain that the goal is not to make the anxiety go away instantly, but to ‘habituate’ to it, much like getting used to cold water in a swimming pool.
They will share the data to help build your confidence in the process. Research confirms that ERP is the most effective treatment available.
- About 75% of adults with OCD experience improvement with ERP.
- In clinical trials, 22.5% showed dramatic improvement, while over 50% showed moderate improvement.
- For many, ERP combined with medication is significantly more effective than medication alone.
You will learn that the ‘Response Prevention’ part, resisting the urge to do the ritual, is where the brain rewiring happens. This is a challenging aspect of ERP therapy, but also the most rewarding.
The Homework: Becoming Your Own Therapist
OCD therapy is a doing therapy, not just a talking therapy. In these early sessions, you will be assigned homework.
This often starts with an OCD Log or Diary. Because OCD is a ‘chameleon,’ constantly changing forms, it is easy to forget specific triggers once you are sitting in the safety of the therapist’s office. You will be asked to jot down:
- The Trigger (What happened?)
- The Obsession (What thought did you have?)
- The Anxiety Level (0-10)
- The Compulsion (What did you do to fix it?)
This log becomes a therapeutic exercise in itself. It forces you to observe the OCD rather than just reacting to it. It also helps you and your therapist set SMART Goals (Specific, Measurable, Attainable, Realistic, Time-based), such as ‘I want to be able to cook dinner without checking the stove more than once.’
Managing Expectations: The Long Game
As you wrap up your first few sessions, your therapist will likely manage your expectations regarding the timeline. Recovery is not a straight line.
If your symptoms are severe, your therapist might suggest a consultation for medication. This is not a failure; it is a strategy. SSRIs (selective serotonin reuptake inhibitors) can help lower the baseline anxiety, making the ERP work more manageable. Since depression co-occurs in half of OCD patients, treating the mood disorder often makes tackling the OCD easier.
You should also expect that you might feel more aware of your symptoms after the first few sessions than when you started. This is known as the ‘therapeutic spike.’ You are finally looking the monster in the eye rather than running from it. This is a sign that the work has begun, not that you are getting worse.
Final Thoughts
Starting therapy is the first step toward reclaiming the time and energy OCD has stolen from you. While the statistics regarding the severity of OCD can be sobering, the statistics regarding treatment are incredibly hopeful.
As Dr. Kim Anderson writes in her 2025 update, ‘These stats can help reduce stigma, validate lived experience and encourage more people to seek the treatment they deserve. OCD is highly treatable, and hope is never out of reach.’
Your first few sessions are about building a safety net, a roadmap, and a partnership. You are no longer alone with your thoughts. You have a plan, you have science on your side, and you have started the journey toward a life defined by your values, not your fears.


